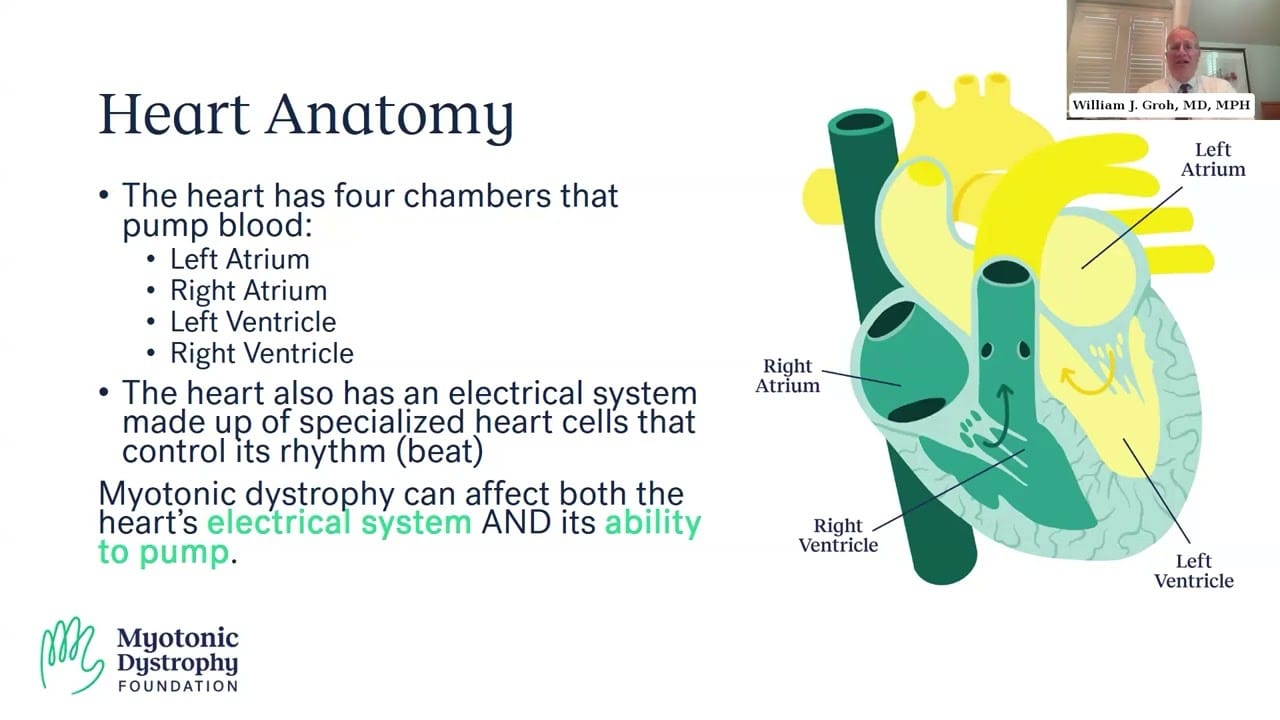
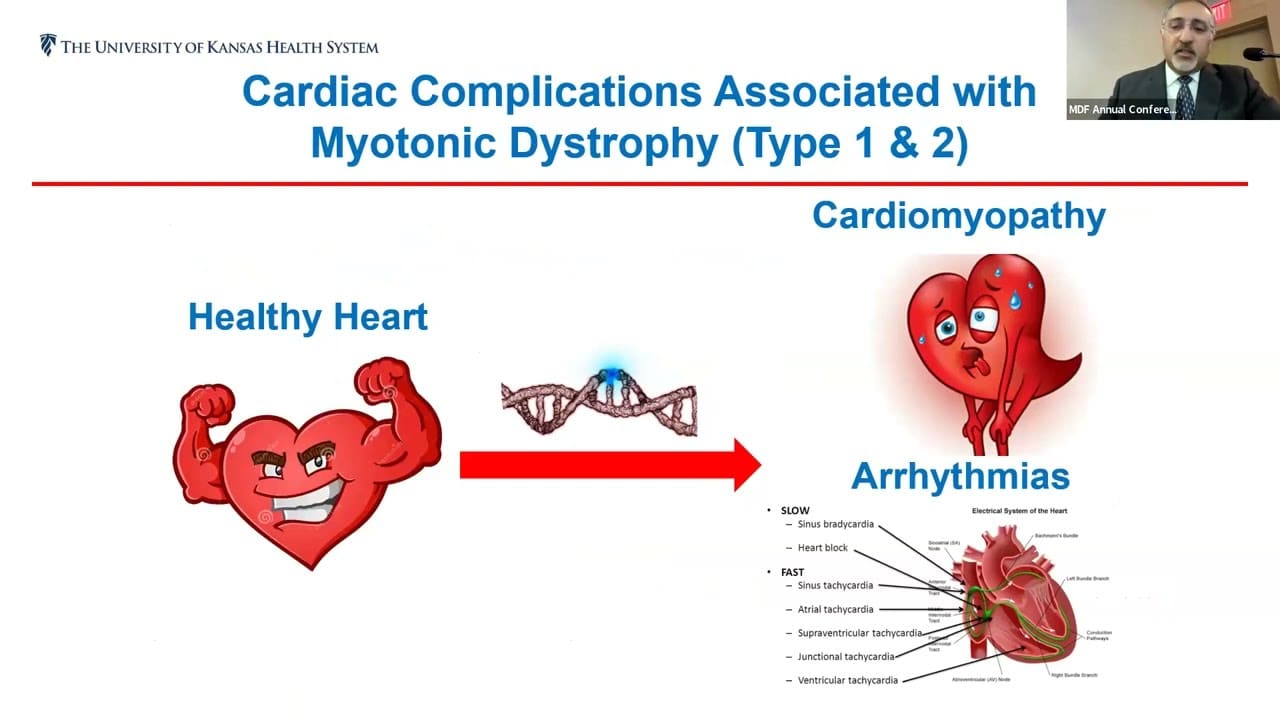
Myotonic dystrophy (DM) can affect the heart, primarily targeting the cardiac conduction system and increasing the risk of arrhythmias. Symptoms may include palpitations, dizziness, fainting, shortness of breath, or chest pain. Both bradyarrhythmias (slow heart rate) and tachyarrhythmias (fast heart rate) are possible, and serious complications such as heart block, cardiomyopathy, or sudden cardiac arrest can occur. Regular cardiac monitoring, including ECGs, imaging, and specialist evaluations, is important. Treatments may include pacemakers, implantable defibrillators (ICDs), medications, and lifestyle precautions to manage arrhythmias and maintain heart health.
Quick facts
Cardiovascular System – DM1
Patterns:
- DM1-related cardiac pathophysiology, although affecting all myocardial tissue, preferentially targets the cardiac conduction system. Conduction system defects are progressive and, while initially asymptomatic, increase the risk for symptomatic arrhythmias.
- Pre-syncope, syncope, palpitations, dyspnea, chest pain or sudden death from cardiac arrest.
- The development of a dilated, non-ischemic cardiomyopathy is an infrequent but recognized occurrence. Once a symptomatic dilated cardiomyopathy is present, progression is typically rapid, with congestive heart failure leading to death.
Symptoms:
- Palpitations, pre-syncope, syncope, dyspnea and chest pain.
- Arrhythmias including sinus bradycardia, tachyarrhythmias, heart block, atrial fibrillation and flutter, and ventricular tachycardia. The most common tachyarrhythmias are atrial fibrillation and atrial flutter, which pose a risk of cardiogenic embolism and stroke.
- Symptom change, abnormal cardiac imaging, abnormal ECG.
Diagnosis:
- Discuss the following tests with your doctor:
- Cardiac testing, including the 12-lead electrocardiogram (ECG), long-term ambulatory ECG monitoring, and an invasive electrophysiological study.
- Imaging studies, including echocardiography, computerized tomography (CT), magnetic resonance (MR), and nuclear imaging can be used to assess the heart’s mechanical status, including left ventricular function.
- Echocardiograph if abnormal ECG indicative of conduction disease or if other symptoms suggestive of heart failure are present.
Treatment:
- Pacemakers can be implanted to treat symptomatic bradyarrhythmias or prophylactically in those at high risk for complete heart block.
- Implantable cardioverter-defibrillators (ICDs) can be installed in those who have survived an episode of a ventricular tachyarrhythmia or, prophylactically, in those at high risk for a ventricular tachyarrhythmia.
- Use of emergency medical alert devices.
- Serial periodic clinical cardiology evaluations.
- Ambulatory Holter ECG monitoring – either short-term (24-48 hours) or long-term (30 days or more) – to detect mechanisms of arrhythmias.
- Mexiletine can provide relief for atrial fibrillation but because it is an anti-arrhythmic, a complete workup must be done first to rule out underlying structural or functional abnormalities that may complicate its use. Mexiletine-related monitoring should be conducted by a cardiologist experienced in the treatment of DM1.
- Refer to:
- A cardiology center experienced in care of DM1.
- An anesthesia practitioner, separate from the operating physician, to provide procedural sedation and monitoring for electrophysiology studies and pacemaker or ICD implantation.
Cardiovascular System – DM2
Patterns:
- DM2-related cardiac pathophysiology, although affecting all myocardial tissue, preferentially targets the cardiac conduction system. Conduction system defects are progressive and, while initially asymptomatic, increase the risk for symptomatic arrhythmias.
- Pre-syncope, syncope, palpitations, dyspnea, chest pain or sudden death from cardiac arrest.
- Risk of both bradyarrhythmias and tachyarrhythmias. The most common tachyarrhythmias are atrial fibrillation and atrial flutter, which pose a risk of cardiogenic embolism and stroke. There is an increased risk of ventricular tachyarrhythmias (tachycardia or fibrillation), a mechanism responsible for cardiac arrest, in DM2.
- Asymptomatic abnormalities are observed in a moderate number of adults with DM2 and are more common in those with conduction system disease.
Symptoms:
- Palpitations, pre-syncope, syncope, dyspnea and chest pain; if observed, seek prompt attention.
- Arrhythmias including sinus bradycardia, heart block, atrial fibrillation and flutter, and ventricular tachycardia.
- Symptom change, abnormal cardiac imaging (MRI or echocardiogram), abnormal ECG.
Diagnosis:
- Discuss the following tests with your doctor:
- Cardiac testing, including the 12-lead electrocardiogram (ECG), long-term ambulatory Holter-ECG monitoring and invasive electrophysiological study.
- Imaging studies, including echocardiography, magnetic resonance (MR), and nuclear imaging to assess the heart’s mechanical status, including left ventricular function.
- Impulse or conduction abnormalities on a standard 12-lead ECG.
- Echocardiography and cardiac MRI if abnormal ECG or other symptoms suggestive of heart failure are present.
Treatment:
- Pacemakers can be implanted either to treat symptomatic bradyarrhythmias or prophylactically in those at high risk for complete heart block.
- Implantable cardioverter-defibrillators (ICDs) can be installed for ventricular tachyarrhythmia, or prophylactically in those at high risk for a ventricular tachyarrhythmia.
- Use of emergency medical alert devices.
- Serial periodic clinical cardiology evaluations; cardiology consultations are recommended in for abnormal electrocardiograms and/or cardiac symptoms.
- Cardiac imaging at diagnosis and every three to five years thereafter.
- Invasive electrophysiology when there is concern about a serious conduction block or arrhythmia because of abnormalities detected via noninvasive cardiac testing.
- Ambulatory Holter ECG monitoring – either short-term (24-48 hours) or long-term (30 days or more) may be considered to detect mechanisms of arrhythmias.
- Refer to:
- A cardiology center experienced in care of DM2
- An anesthesia practitioner, separate from the operating physician, to provide procedural sedation and monitoring for electrophysiology studies and pacemaker or ICD implantation.
Cardiovascular System – CDM
Patterns:
- DM1-related cardiac pathology manifests predominantly as arrhythmias due to progressive abnormalities in the conduction system of the heart. Clinical presentations may include: presyncope, syncope, palpitations, dyspnea and, rarely, chest pain or sudden death from cardiac arrest.
- Bradyarrhythmias (arrhythmias that cause a slowing of the heart rate) are not reported in literature under the age of ten years. Rarely, life-threatening tachyarrhythmias have been reported as young as ten. Although exact numbers of sudden cardiac death in children with DM1 or CDM are not known, they are thought to be very low.
Symptoms:
- Symptoms representing arrhythmias, sinus bradycardia, heart block, atrial fibrillation and flutter, orventricular tachycardia on ECG and systolic dysfunction on echocardiogram.
- Symptom change, abnormal cardiac imaging, abnormal ECG.
- Palpitations, dizziness, syncope, non–sinus rhythm.
Diagnosis:
- Discuss the following tests with your doctor:
- Evaluation of severity of cardiac rhythm disturbance via a 12-lead electrocardiogram (ECG), and long-term ambulatory ECG monitoring.
- Serial ECG studies are useful to follow progression of conduction system abnormalities over time, as they are often asymptomatic.
- Transient arrhythmia via 24-48 hour ambulatory holter ECG monitoring. Longer monitoring if the 12-lead ECG is abnormal or if symptoms are suggestive of an arrhythmia.
- Cardiology evaluation with examination, ECG, echocardiogram, and ambulatory electrocardiographic monitoring should occur at the time of DM diagnosis, regardless of symptoms.
- For individuals with normal LV ejection fraction and no evidence of the symptoms described prior, it is reasonable to reassess by examination, ECG, and ambulatory electrocardiographic monitoring annually and by echocardiogram every 2 to 4 years.
Treatment:
- Use of emergency medical alert devices to identify DM1 diagnosis and risk of arrhythmia.
- Be informed about the risks of arrhythmias and cardiac dysfunction and the importance of prompt medical attention if symptoms are observed (i.e. palpitations, pre-syncope, syncope, dyspnea, chest pain, unexplained fatigue).
- Serial periodic clinical cardiology evaluation; specialist cardiology consultations are essential with abnormal electrocardiograms or cardiac symptoms.
- Refer to:
- In-hospital cardiac monitoring to detect arrhythmias if admitted for longer duration than typical following surgical procedures.
- In-hospital cardiac monitoring if admitted due to severe illness or infection.
Related videos

Keeping Your Heart in Check: DM1’s Impact and Care Tips - 2025 MDF Conference
Published: August 28, 2025
How Myotonic Dystrophy Affects the Heart - 2024 MDF Regional Conference in Los A...
Published: September 14, 2024
Ask-the-Expert: Myotonic Dystrophy & the Heart
Published: July 29, 2024
Cardiac Considerations for Myotonic Dystrophy Type 2 - 2023 MDF Annual Conferenc...
Published: November 21, 2023