Myotonic dystrophy (DM) can weaken the muscles used for breathing and swallowing, including the diaphragm, chest, and abdominal muscles. This can lead to low oxygen, high carbon dioxide, ineffective cough, sleep disturbances, aspiration, and recurrent lung infections. Respiratory complications are a major cause of illness and mortality in DM1. Diagnosis may involve lung function tests, sleep studies, and airway assessments. Management can include airway clearance techniques, cough assistance, vaccinations, noninvasive ventilation, mechanical ventilation when needed, and specialist pulmonary care. Children with congenital DM may have early respiratory weakness, while severity varies across DM types.
Quick facts
Respiratory System – DM1
Patterns:
- Significant breathing problems that can result from muscle weakness of the diaphragm, abdominal and intercostal muscles and myotonia of these muscles.
- Low blood oxygen and elevated blood carbon dioxide levels.
- Chronic respiratory impairment is the primary cause of mortality and morbidity in DM1.
Symptoms:
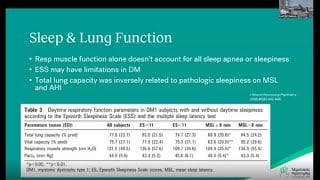
- Excessive daytime sleepiness (EDS).
- Insufficient air flow during sleep.
- Weakness of the breathing and swallowing muscles.
- Aspiration of food and drink, saliva, nasal secretions and stomach fluids.
- General anesthesia and pain medications, especially opiates, often cause respiratory failure.
- Ineffective cough.
- Recurrent chest infections.
- Morning headaches, apnea, snoring.
Diagnosis:
- Discuss the following tests with your doctor.
- Forced vital capacity (FVC) and forced expiratory volume.
- Respiratory muscle strength evaluation.
- Sleep study.
- Clearance capacity.
Treatment:
- Careful perioperative management.
- Vaccinations for influenza and pneumonia if no contraindications.
- Respiratory cough assistance and mechanical ventilation (as needed).
- Consultations from respiratory therapy and pulmonary medicine groups as needed.
- Airway clearance and lung volume recruitment techniques (e.g., breath stacking, abdominal thrust, the vest and the mechanical insufflator/exsufflator).
- Noninvasive positive-pressure ventilation (NIV) for respiratory insufficiency.
- Emergency medical alert devices.
Respiratory System – DM2
Patterns:
- Significant breathing problems that can result from muscle weakness of the diaphragm, abdominal and intercostal muscles and myotonia of these muscles.
- Poor ventilatory force, low blood oxygen and elevated blood carbon dioxide levels.
Symptoms:
- Fatigue, excessive daytime sleepiness (EDS) and respiratory failure.
- Insufficient air flow during sleep may contribute to disrupted sleep.
- Weakness of the swallowing and breathing muscles.
- Aspiration of food and drink, saliva, nasal secretions and stomach fluids.
- General anesthesia and intravenous pain medications, especially opiates, can cause respiratory failure.
- Ineffective cough.
- Recurrent pulmonary infections.
- Frequent chest infections.
- Morning headaches, apnea, fatigue and snoring.
Diagnosis:
- Discuss the following tests with your doctor:
- Sleep study
- Respiratory tests
- Clearance capacity
Treatment:
- Careful perioperative management.
- Vaccinations for influenza and pneumonia if no contraindications.
- Respiratory cough assistance and mechanical ventilation (as needed).
- Consultations from respiratory therapy and pulmonary medicine groups as needed.
- Airway clearance and lung volume recruitment techniques (e.g., breath stacking, abdominal thrust, the vest).
- Nighttime ventilatory support and full-time ventilation.
- Supplemental oxygen.
- Emergency medical alert devices.
Respiratory System – CDM
Patterns:
- Most children with childhood-onset myotonic dystrophy have normal breathing function and few respiratory issues. However, the spectrum of severity is wide, and some children with DM1 may have significant breathing problems resulting from muscle weakness of the diaphragm, abdominal and intercostal muscles.
- Weakness is common in CDM, and respiratory failure in the neonatal period is often a presenting feature and a significant cause of morbidity.
Symptoms:
- Weakness of the inspiratory and expiratory muscles.
- Impaired clearing of secretions.
- Pulmonary infections and to aspiration of material into the lungs.
- Excessive daytime sleepiness (EDS) and respiratory failure.
- Disrupted sleep, morning headaches, apnea and snoring.
- Restless leg syndrome.
- Ineffective cough.
Diagnosis:
- Discuss the following tests with your doctor:
- Forced vital capacity (FVC) and forced expiratory volume
- Sniff nasal inspiratory pressure (SNIP) test
- Nocturnal oximetry if snoring, nightly interrupted sleep, morning headaches or excessive daytime sleepiness are present
- Peak expiratory flow during cough
- Sleep study if symptoms of snoring, nightly interrupted sleep, morning headaches or excessive daytime sleepiness are present
- Clearance capacity and other respiratory assessments prior to surgery
Treatment:
- Vaccinations for influenza and pneumococcus pneumonia.
- Standard medical therapy as soon as possible for respiratory infections, including respiratory cough assistance and mechanical ventilation as needed.
- Consultations from respiratory therapy and pulmonary medicine group.
- Cough assistance techniques (e.g., air stacking, abdominal thrust and cough machine).
- Noninvasive positive-pressure ventilation (NIV) for respiratory insufficiency.
- Emergency medical alert devices or wallet cards.
Related videos

Breathe Easy, Sleep Sound: Managing Sleep and Pulmonary Health with DM1 - 2025 M...
Published: August 28, 2025
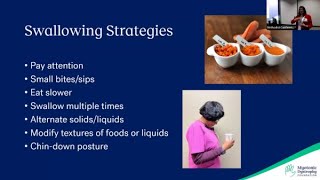
Nutrition and Swallowing in Myotonic Dystrophy - 2024 MDF Regional Conference in...
Published: September 14, 2024
Beyond the Muscle: Navigating Sleep & Pulmonary Challenges in Myotonic Dystr...
Published: September 13, 2024